You’ve got the medical records. You’ve reviewed every progress note, every medication administration record, every physician order. But here’s what most attorneys miss: the smoking gun isn’t always in the chart.
It’s hiding in the staffing records.
While everyone’s focused on what happened to the patient, we’re looking at who was there when it happened, and more importantly, who wasn’t. Because the best-documented care plan in the world means nothing when there’s nobody qualified to execute it.
The Records Defense Attorneys Don’t Want You to Request
Staffing records tell a story that clinical documentation deliberately avoids. They reveal the operational chaos that creates the perfect storm for negligence.
When you subpoena these documents, you’re not just getting names and shift times. You’re getting evidence of systemic failure.
Here’s what you should be demanding in discovery:
- Master staffing schedules for the 90 days surrounding the incident. Not the “official” schedules, the actual ones showing who called out, who got pulled to another unit, and who worked a triple shift because nobody else was available.
- Time and attendance records that reveal patterns. When the same CNA is working 16-hour shifts six days a week, you’ve found your exhaustion-related error waiting to happen.
- Personnel files for every staff member who touched your client. Licenses, certifications, disciplinary actions, performance reviews. That nurse who missed the sepsis? Check her file. She might have three prior write-ups for missing critical changes in patient condition.
- Orientation and training documentation. Was the nurse who administered the wrong medication even competent in that medication? Did she complete the required training? The absence of documentation is documentation.
- Agency staffing contracts and invoices. They’re using travelers and agency nurses because they can’t keep permanent staff. That tells you something about the facility, and it tells a jury even more.
What the Numbers Actually Reveal
Raw data becomes evidence when you know how to read it.
A nursing home claims they maintain proper staffing ratios. Their policy manual says one nurse for every 15 residents during day shift. Sounds reasonable on paper.
Then you analyze three months of actual staffing records and discover they hit that ratio maybe 60% of the time. The other 40%? One nurse covering 25 residents. On the day your client developed that Stage 4 pressure ulcer, it was one nurse and one CNA for 30 residents.

That’s not negligence. That’s a mathematical impossibility masquerading as care.
We calculate actual nurse-to-patient ratios for every shift in question. We identify coverage gaps. We document when mandatory overtime created unsafe conditions. We show patterns that prove the incident wasn’t an isolated mistake; it was inevitable.
Here’s what defense attorneys hate: staffing records can’t be edited after the fact, like progress notes can. The payroll system doesn’t lie. When someone clocks in and clocks out is documented in multiple systems. You can’t “amend” the fact that nobody was on the floor for 45 minutes during shift change.
The Red Flags We Hunt For
Chronic short-staffing patterns show institutional knowledge of the problem. When a facility consistently operates below safe levels, it has made a business decision to prioritize profit over patient safety. That’s not an accident. That’s corporate negligence.
Excessive use of agency or travel nurses indicates a crisis facility. High turnover means staff who don’t know the patients, don’t know the facility’s systems, and don’t have relationships with the physicians. Care quality suffers. Errors multiply.
Unqualified staff performing skilled tasks. We’ve seen CNAs giving medications because “the nurse was too busy.” We’ve seen medical assistants performing wound care that they weren’t trained or licensed to do. The chart might say “nurse provided care,” but the staffing records show the nurse was in another building.
Scheduling gaps during critical times. That fall at 6:30 AM? There was no night shift CNA because she left at 6:00, and the day shift CNA didn’t arrive until 7:00. Nobody told the family their loved one would be completely unsupervised during the highest-risk time of day.
Disciplinary patterns among staff involved. When you pull personnel files and discover that three of the four staff members involved in your case had prior write-ups for similar issues, you’ve just established that administration knew they had problem employees and kept them on the floor anyway.
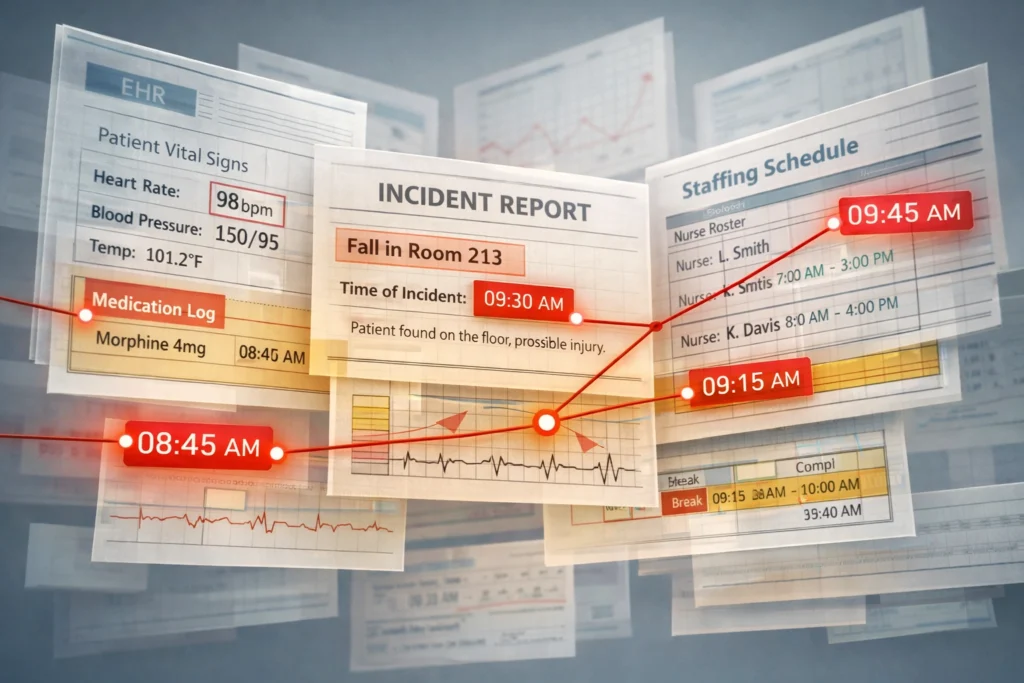
How We Connect Staffing to Outcomes
The magic happens when we overlay staffing data with incident reports and patient outcomes.
A hospital claims the medication error was an isolated incident by an otherwise competent nurse. Then we show that in the six weeks before the error, the nurse worked 18 shifts over 14 days, including four double shifts. She was averaging 60 hours a week when the error occurred on hour 14 of her shift.
Suddenly, it’s not about one nurse’s mistake. It’s about a facility’s staffing practices that guarantee mistakes will happen.
We create timelines that demonstrate cause and effect. We calculate actual staff-to-patient ratios at the moment of the incident. We identify which tasks couldn’t have been completed given the staffing levels present.

When the chart says “patient monitored every two hours,” but the staffing records show it was physically impossible for one nurse to monitor 20 patients every two hours while also administering medications, answering call lights, and documenting, you’ve got proof the documentation is fiction.
The Questions These Records Answer
Can the facility’s documentation be trusted? When staffing records contradict the clinical notes, something’s wrong. If the chart says a wound was assessed and dressed at 2:00 PM, but the only nurse on duty was in surgery with another patient, the chart is lying.
Was the staff adequately trained? Personnel files reveal whether required certifications were current. A facility can’t claim its nurses were competent when half of them hadn’t completed their annual competency assessments.
Did management know about the problem? When you find emails, incident reports, or staff meeting minutes discussing chronic staffing shortages, you’ve proven knowledge. They knew. They did nothing. That’s institutional negligence.
Could this have been prevented with proper staffing? Almost always, yes. Most adverse events in healthcare settings are directly linked to understaffing, fatigue, or inadequate training: all of which show up in staffing records.
Why Defense Attorneys Fight These Requests
They’ll object to staffing record requests as overly broad, burdensome, or not relevant to the case. They’ll offer to provide “summaries” instead of raw data.
Don’t accept summaries. Don’t accept their narrative about staffing levels.
Defense counsel knows what we know: staffing records transform a case from “one bad nurse” into “systemic negligence by administration.” They shift liability from an individual to an institution. They demonstrate knowledge, pattern, and profit motive.
That’s why they fight so hard to keep these records out of your hands.
The Bottom Line
Medical records tell you what happened. Staffing records tell you why.
While other attorneys are focused exclusively on clinical documentation, we’re building the bigger picture. We’re showing juries that the patient didn’t just have bad luck with one careless nurse. They were harmed by an institution that chose profit margins over patient safety.
The evidence is there. It’s in the scheduling software, the payroll system, the personnel files, and the time cards. You just need someone who knows where to look and how to interpret what they find.
At OnPoint Legal Nurse Consulting, we don’t just review medical records: we investigate the systems that failed your client. We turn administrative data into compelling evidence. We find the negligence that isn’t written in the chart.
Because sometimes the most important witness isn’t a nurse or a doctor. It’s a spreadsheet showing nobody was there at all.
Ready to dig deeper into your case? Let’s talk about what the staffing records might reveal.